
Newsletter One + Patient Zero
Shall we begin?

Hello everyone - welcome to the first issue of Out of Pocket! Excited to traverse the greenfield of healthcare analysis and comedy, and glad you’ve decided to join me.
Alright, let’s get after it.
Coronavirus
I didn’t want my very first issue to be about this, but here we are. As per usual, instead of listening to actual experts, my friends keep asking if they should be worried about COVID-19. To remind everyone, to the sadness of my parents I am not a doctor or public health person, just a thinkboi. But I figured I would just put this down in a newsletter.
Things I know:
I am not an expert on this.
You should listen to actual experts on this and not vigilante epidemiologists on Twitter. Spreading misinformation is exactly how sh*t is going to hit the fan and makes it difficult to organize a coordinated response. In fact I would say it’s a history of fear mongering and misinformation around public health issues that’s made the public extremely confused about when they should be very seriously preparing. A true “boy who cried wolf” scenario taking place.
Every government has been extremely terrible at releasing information, which creates a void that people ended up filling with misinformation.
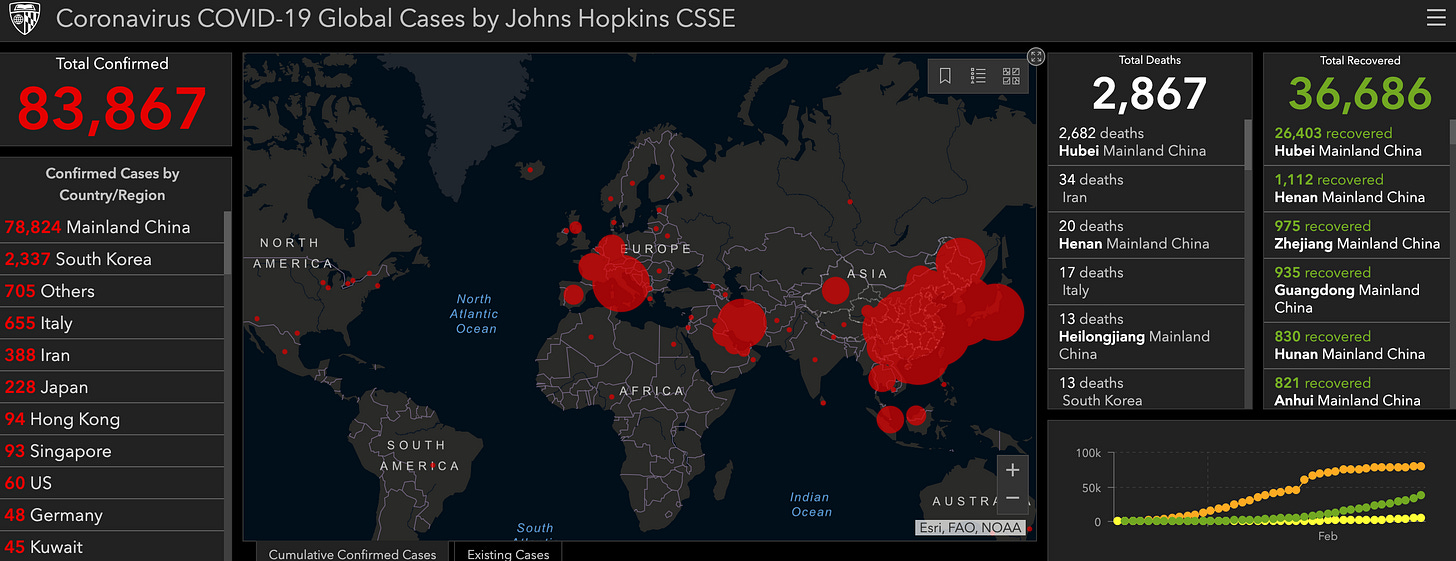
There are about ~83K reported cases and ~3K reported deaths. This is now spreading across the world and you should at least think about having 30-day stocks of medicines and food just in case. There’s a great interactive map from JHU showing the spread, and they decided to use the most intimidating color scheme possible.
Also keep washing your hands! And if you’re sick or elderly, take extra precautions.

Things I don’t know:
What the appropriate response should be going forward from governments.
Whether you are personally at risk for getting the coronavirus and if you’ll survive. This is mostly a risk for people with existing conditions and the elderly. But there have been deaths of healthy young adults too including the doctor who sounded the alarm, so idk.
Why stocks are moving in certain directions. For the drug companies, addressing this situation isn’t good business for them (more on this below). For remote work tools like Zoom, the pricing and utilization likely won’t change post outbreak. All of this seems like pseudo-intellectualized gambling.
Why did the CDC put out this absolutely hilarious graphic? Since when did THAT mustache get called a toothbrush??? Why didn’t they just outline where to NOT have facial hair instead of create every permutation of facial hair?

So in summary - this newsletter is not a good place to get your information about this! All I can tell you is that I bought like 15 lbs of chicken to freeze just in case, so if this doesn’t turn out to be a thing then I have a lot of slow cooking to do.
However, I hope people that don’t get the flu shot each year or poop with their phone think a bit about the irony that they’re freaking out about coronavirus and taking massive measures to protect themselves.
Climate Change
I was on a podcast a few months ago (flex) with my friend Malay Gandhi, and he started talking about how healthcare opportunities are going to open up thanks to things like climate change (around 1:22:00). His response when asked about the opportunities in climate change + healthcare were (my annotations in bold italics):
Malay: *Hits joint* "Like infectious diseases is probably the clearest example, the craziest stuff would be adaptability solutions even for humans to survive as the climate changes. Like are there things we can do to modify our environments, where our biology is better adapted to that environment or we adapt the environment around our existing biology.
At first I thought this was some futuristic Animorphs nonsense. But the more I think about this, the more prescient I think this is. The global response to COVID-19 gives an example of situations we’ll need to be prepared to respond to.
Here are some lessons from this outbreak and the potential healthcare opportunities/changes to think about in a climate changing future.
Development Incentives - If we expect to be ready for pandemics and infectious disease being a global burden again, we need to have a better incentive system for new vaccine/antibiotic development for infectious disease. Currently the R&D for vaccines and antibiotics is expensive and the ability to recoup the investment is terrible because it’s difficult to price them high, the frequency of use is very low and sporadic, and it’s hard to stockpile them in many cases. To make matters worse, for antibiotics the efficacy can become much worse over time and for vaccines the manufacturing process is relatively complex.
Running a clinical trial for vaccines and antibiotics is also difficult (especially in mild-to-moderate cases) because it’s hard to recruit for a trial when an outbreak isn’t happening and difficult to figure out whether the drug or your immune system did the work.
What Moderna Therapeutics is doing with its new COVID-19 vaccine is really interesting to watch. They use an mRNA-based vaccine, which are new and very promising because they can be produced in labs quickly and cheaply instead of needing complex manufacturing (perfect for outbreaks).
But this would still take years to get to market. For reference, the ebola vaccine was approved this past December, several years after the outbreak subsided.
There needs to be new incentive models to make innovation in the vaccine and antibiotic space more regular (global bounties?). What if we just reframed the problem…
Point of care pathogen detection: One of the biggest failings of this entire coronavirus saga is that we haven’t been doing widespread diagnostics of people that are potentially infected in the US, even in hospitals where the most at-risk people are. One reason is because only a handful of labs were authorized to run the test for coronavirus, and every other lab (even ones that are really good) have to apply for an “emergency use authorization”. The CDC also sent a bunch of kits with a bad ingredient, which delayed things even more.
Beyond the US, labs that can test for the virus get overwhelmed with the number of samples and require equipment like PCR machines which might not be readily available in rural areas.
Being able to do diagnostics at-scale is important not only to treat patients, but also to understand the spread of a disease across the country. This requires a massive amount of coordination and data-sharing, things the healthcare system absolutely despises.
I’d like to see more investment in diagnostics that happen near the patient (point-of-care) instead of ones that have to travel to a lab. The science of this goes way over my head but companies like Mammoth Biosciences or some of the nanopore sequencing companies like Oxford Nanopore could hopefully be useful here? Would also be interesting to see if health trackers (Apple Watch, etc.) can detect faint changes in your heart rate/autonomic nervous system that might suggest you have an issue earlier based on data from other coronavirus patients.
Telemedicine: Telemedicine is finding a surge in demand. In China, Alipay saw 300M people use their telemedicine services from FEBRUARY (sometimes you have to take these numbers with a grain of salt, because the definition of “use” can get really loose).
In many non-US countries with high patient:physician ratios, telemedicine as the first visit is becoming more normalized. In the US, telemedicine adoption is low even though you can get a lot of issues resolved via telemedicine alone, or at least they can tell you if you need to see a doctor in-person. I wonder if coronavirus becomes a catalyzing event where people use telemedicine, enjoy the experience, and then start going to telemedicine first instead of a clinic. There’s a separate newsletter to be written about whether the telemedicine economics for an outbreak or good or bad.
I also still laugh to myself about this Oscar ad from years ago. People won’t get their pink-eye checked out on the phone, but yeah maybe they’ll do this.

Front-line Robots: We need robots to do this front-line care. We’re putting so many people at-risk because we don’t have proper protective gear for the people taking care of these patients. Maybe instead of pizza-making robots or whatever, a better use case would be assisting containment. Softbank where you at?
Delivery Robots: Beyond just taking care of patients and interacting with them, in areas where road infrastructure is bad there’s going to be a huge problem delivering healthcare goods in a timely manner (especially if climate change related disasters become more frequent). Drone delivery is being used for life-saving materials like blood, but you can imagine in the future it becomes more normal to drop materials into hard to reach areas.

Animal Control + Health - Many of these pandemic-prone outbreaks start in the food chain somewhere. Being able to either detect these issues earlier with better diagnostics OR manipulating the DNA of livestock for better immunity against viruses and bacteria is key to preventing the jump into humans. I’m sure this will go over well with the anti-GMO crew.
Additionally, some climate scientists predict that warmer weather across the globe will expose many more people to mosquitos and the diseases that come with them. Luckily, the most likely suspects are tackling the issue, like…Google…?
I’m very excited to explain to my kids in 50 years how a search engine ended up eradicating the West Nile Virus.

That’s a wrap for issue #1! Slowly getting back into the writing/analysis groove. Hope you enjoyed it and let me know if there’s anything you agree/disagree with. If there are future areas you want me to tackle or look into let me know.
"thinkboi" Where as this word been all my life?!
The worlds first infodemic is here