


The Issue With The COVID Bailout
A WHOLE NEW WORLD, A NEW PANDEMIC POINT OF VIEW


Hello - I’ve started an instagram for Out Of Pocket. It’s mostly going to be me making more memes about healthcare. I also have no idea how to “be good” at Instagram so any tips are appreciated :).

Hospital Consolidation
Jumping off of my rant about non-profit hospitals, I want to kick things off by talking about hospital consolidation.
What do you think is the most expensive part of US healthcare? The answer is hospital care. Hospital care alone is 1/3rd of all healthcare expenditure in the US.

There are lots of possible reasons that hospital care is the biggest chunk. Maybe it’s because hospitals spend so much on administrative costs. Maybe it’s because we have too many specialists that get paid a lot. Maybe it’s because we consume more healthcare as a nation. Each of these is a newsletter in itself.
The one I really want to focus on is hospital consolidation which has led to pricing increases. In the last 12 years, hospitals been getting scooped up left right and center.

A lot of this was by design. The Affordable Care Act (ACA) made it way more difficult to be a independent, physician-owned practice by increasing the amount of regulatory + administrative requirements to remain independent and lowering the amount they would get from reimbursement.
The predominant belief was hospitals would give patients better care if they controlled the full patient journey and used their economies of scale to reduce prices. You know, the same way that group projects become easier when you keep adding people, and other industries see their prices go down when there are only 1-2 viable options to choose from. Right…?
Dr. Bob Kocher, one of the architects of the ACA, admitted this was probably an incorrect assumption (which I respect a lot and wish more people in government did).
“What I got wrong about ObamaCare was how the change in the delivery of health care would, and should, happen. I believed then that the consolidation of doctors into larger physician groups was inevitable and desirable under the ACA. I joined my White House health-care colleagues—Ezekiel Emanuel and Nancy-Ann DeParle—in writing a medical journal article arguing that “these reforms will unleash forces that favor integration across the continuum of care.” We added that “only hospitals or health plans can afford to make the necessary investments” needed to provide the care we will need in a post-ACA world.” -Bob Kocher
What ended up happening was hospitals formed local monopolies in their geographies. Many practices ended up selling or affiliating themselves with large hospital systems. There are no longer geographies that have strong competition for health services - it’s become reduced to duopolies and triopolies.

So what happens when hospitals start becoming local monopolies? Shockingly, prices go up significantly compared to competitive markets almost immediately after consolidation happens.

But I guess we’re paying more for better quality care. Actually lol jk care quality is probably the same and actually sometimes worse. Verdict is still out on this one.
The study, published in Health Services Research, focused on the health care outcomes of about two million Medicare beneficiaries who had been treated for hypertension, for a cardiac ailment or for a heart attack from 2005 to 2012.
The study found that when cardiology markets are more concentrated, these kinds of patients are more likely to have heart attacks, visit the emergency department, be readmitted to the hospital or die. These effects of market concentration are large. [Nikhil’s note: YOU HAD ONE JOB!!!]
I firmly believe reversing hospital consolidation and making physicians more independent is one of the core ways we can reduce healthcare costs in the country.
Bail Money
The consolidation topic is once again in the spotlight as the government assesses how to shell out the bailout money. If you were to guess who could distribute $100B faster and more haphazardly, would you put your money on SoftBank or the government? We’ll get to see!

At a time when most independent physician practices are already struggling to stay independent, we now have a pandemic which kneecaps them. Patient visits are down ~60-65%. While many of these practices try to do what they can with their remaining patients through telemedicine, this is still reimbursed less than an in-person visit + doctors can’t do many things via telemedicine like procedures that would actually make the practice money.
Large hospitals are getting slammed and overcrowded. They’ve also been forced to shut down a lot of the revenue generating parts of their businesses, specifically elective surgeries (aka. surgeries you can shop around and plan in advance). Large hospitals are losing lots of money too.
The difference is that when the bailout dollars are distributed, I can bet that the lion’s share is going to large hospitals that employ a lot of people, want to be reimbursed for providing COVID care, and can demonstrate that they were saviors in their communities. This actually isn’t wrong at all - but in some ways it’s a byproduct of consolidation that we’re entirely reliant on them.
But my guess is that COVID is a nail in the coffin for the physician-owned practice when the dollars don’t make it to them. Many doctors are going to retire, many practices are going to shutter permanently, and many are going to sell for cheap.
A lot of private practice owners are above 55. Retirement hits different once you can touch that Roth IRA money.

Some ground rules for hospitals
What I’d like to see is at least some provisions around the money that’s going to inevitably be doled out to large hospitals. Right now the government has a ton of leverage, and should use it to get some guarantees out of these hospitals. Specifically, I’d like to see:
More mandates around hospitals creating standardized APIs and meeting the data interoperability timelines the Office of the National Coordinator for Health IT (ONC) has set.
End the concept of surprise billing - it’s absolutely nonsensical that we have a system where a hospital can be in-network but a physician can be out-of-network.

Re-evaluate the non-profit status completely, which I already went into in detail.
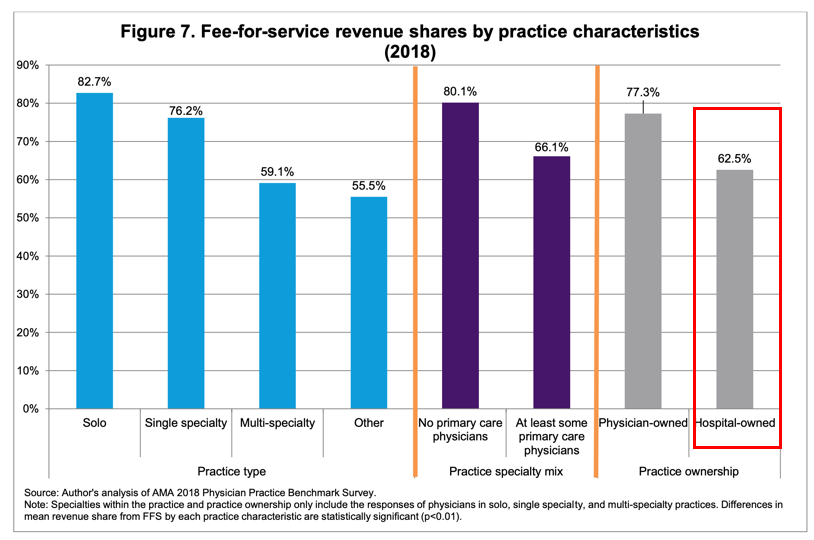
Force hospitals into more risk-based contracts - right now a majority of revenue at hospitals still come from fee-for-service contracts where hospitals are paid based on the volume of services instead of the quality/outcomes of services.

Direct cash infusions to front-line workers that put themselves in harms way to take care of patients.
The new era of practices
While I think the outlook for current practices looks bleak, I actually think the new era of independent practices will emerge out of this. Some guesses:
More telemedicine-native practices instead of telemedicine as an add-on. A company I advise, DocSpace has been working on this problem for a while. They bring the costs of starting a practice way lower, by letting physicians build virtual private practices first before moving into the real-world.
Practices with limited space requirements. This can be in the form of extremely small, low overhead micro clinics. This can be mobile clinics. Or it can be more flexible space agreements where doctors lease space “as needed”.


More practices that get a majority of their revenue in capitated plans (aka. where you get paid a flat fee per patient you take care of based on estimate of how risky they are). I think we’ll discover that practices that were getting more revenue from these kinds of arrangements did better during COVID.
Insurance is going to get more involved and start buying practices. Insurance companies probably have quite a bit of cash right now since a lot of really expensive surgeries were canceled. We’re already starting to see signs of practices selling to insurers (e.g. Blue Shield just bought a 2,700 physician group called Brown & Toland).
Private equity will work with certain physicians to spinout/create joint-venture independent practices in procedure-heavy specialties that were likely impacted hard during COVID. This could also happen in particularly at-risk patient groups too, similar to what we saw with PE firm Welsh Carlson and Humana spending $600M to create Medicare specific primary care clinics.
I’m hoping that future regulation makes it easier for new practices to start and small businesses to be supported. Post-COVID, we need to have a real conversation of how dominant large hospitals have become and how they contribute to cost increases.
Thinkboi out,
Nikhil aka. Probably Could Use A Bailout
Twitter: @nikillinit

If you’re enjoying the newsletter, do me a solid and shoot this over to a friend or healthcare slack channel and tell them to sign up. The line between unemployment and founder of a startup is traction and whether your parents believe you have a job.
So well explained - those of us who have been patient (ailing victim) players in this “not for profit” healthcare heist, appreciate seeing our hunches in print. Yes, that is what we felt was being foisted upon us - but we’re too sick, vulnerable or grief stricken to challenge. Thank you for spelling it out for us.